

|
Source: Cannabis Health vol 2, Issue 1 by Willem K. Scholten Willem K. Scholten PharmD. MPA, is head of the Office of Medicinal Cannabis of the Ministry of Health, Welfare and Sport, The Hague, The Netherlands.
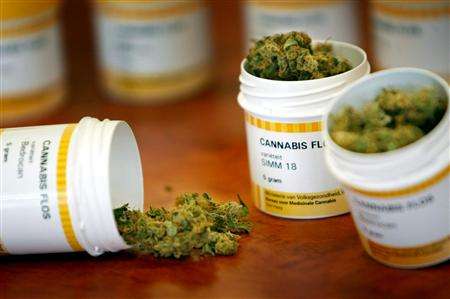
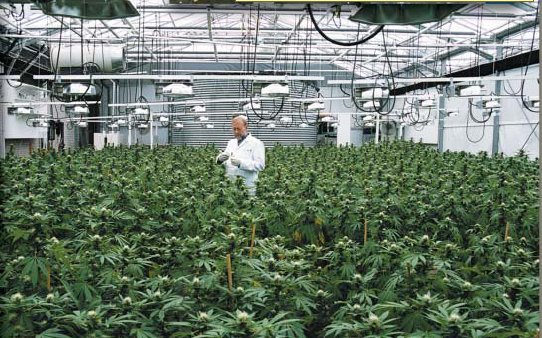
Cannabis has been available on prescription in the Netherlands since the 1st of September 2003. Following a government decision taken in autumn 2001, preparations were made to cultivate and distribute cannabis under government control. After tendering, the Office of Medicinal Cannabis (OMC) contracted two growers, a laboratory, and a packaging and distribution company. Cultivation started last March and the first batches were ready for sale in August. The OMC is a government agency with a monopoly on the wholesale of cannabis. It is also responsible for granting any licences required for cannabis or cannabis resin. The fact that it holds the monopoly means that all cannabis is owned by the state from the moment the harvest is bought from the growers until the final product is sold to a pharmacy in sealed five-gram containers. The contracted growers, the Institute of Medical Marihuana (SIMM) and Bedrocan, are required to comply with the rules of Good Agricultural Practices (GAP) for the cultivation of medicinal cannabis. These rules were laid down by the Dutch Minister of Health, Welfare and Sport and are based on the GAP rules formulated by the European Agency for the Evaluation of Medicinal Products. Additional rules were introduced to standardise the cultivation and drying processes and to prevent diversion. Standardised cultivation ensures a constant cannabinoid content in cannabis products. As the two growers employ different methods and cultivate different varieties, their end-products differ from one other. As a result, prescribers and patients are offered a choice of products. The Bedrocan variety contains approximately 18 percent dronabinol (the official WHO designation for THC) and the SIMM 18 variety around 15 percent. Both are low in cannabidiol. The OMC is considering expanding the product line in future by adding varieties with a higher cannabidiol content or a high cannabichromene or cannabigerol content.
The cannabis is laboratory tested for identity, purity and content, using an analytical monograph drafted by the National Institute for Health and the Environment (RIVM). It is tested to ensure purity from microbiological contamination, heavy metals and pesticides, and to establish the dronabinol, cannabinol and cannabidiol content. Finally, it is packed in polypropylene containers holding five grams each. We made grateful use of Canadian documents when designing our quality control system. They prevented us from overlooking important factors and helped us to harmonize production and international quality requirements right from the start. On the basis of the laboratory results, the OMC approves batch release for packaging and distribution. The company responsible for packaging also does the logistics on behalf of the government, taking orders by phone, fax or email and forwarding them to pharmacies within 24 hours. It invoices customers monthly and collects payments on behalf of the OMC. Cannabis is supplied only to pharmacies; patients cannot order it themselves. Dutch policy is based on the principle that cannabis is a medicine, like morphine or any other controlled narcotic. Hence, there is no reason to prohibit its use for medicinal purposes as long as it is prescribed according to the rules that apply to all controlled substances and that it is used in a responsible manner. We refer to our products as cannabis or hemp (hennep in Dutch). We choose not to use terms like ‘weed’ and ‘marihuana’, which are associated with the recreational use of drugs and may stigmatize patients as drug abusers. The product information provided by the OMC notes that the efficacy of cannabis has not yet been proven, although it is recorded as a treatment for over 200 conditions. It should therefore be used only if the conventional treatments prescribed in medical protocols prove ineffective, and not as a first-line treatment. In other words, it is indicated only if other drugs offer insufficient relief or produce excessive side effects. In the Netherlands cannabis is recommended only for the conditions listed below, for which there is most evidence of its efficacy:
Under Dutch law, doctors are not prohibited from prescribing cannabis for other conditions, but they are answerable to the medical council or the health care inspectorate for any adverse effects. The Netherlands is thus following the example set by Canada, where cannabis has been used for medicinal purposes for some years. Though not identical, the policies of the two countries are similar in many respects. Above all, both recognise the medical potential of cannabis but require more evidence of its efficacy. In the meantime, Canada has allowed cannabis to be used on compassionate grounds, but without giving it medical status. The Netherlands allows doctors to prescribe it as a last-line medicine. Both countries encourage research. Few clinical trials were carried out during the decades of worldwide prohibition, and information is sorely needed. As explained below, Canada has so far been more successful than the Netherlands in generating research. Canada and the Netherlands are the first and, at present, the only countries to allow the medicinal use of cannabis, and both have to do the groundwork. This may change in the future, as several other initiatives have been launched. The UK-based company GW Pharmaceuticals plc, for instance, has developed a sublingual spray based on a cannabis extract. It has applied to have it licensed in the UK. The government of New South Wales in Australia recently announced its intention to make cannabis available for clinical trials on a relatively large scale. Cannabis will be supplied to all patients suffering from certain specified conditions. Several European countries, including Belgium, Germany and Luxembourg, are reconsidering their positions and may ultimately accept cannabis as a useful medicine. Some patients in Canada are evidently dissatisfied with the distribution of cannabis in their country and are under the impression that the Dutch are doing better. However, they may be overlooking the fact that the Canadian government authorised the possession, cultivation and use of medicinal cannabis several years ago. The Netherlands followed suit only as of 1 September 2003 by making it legal to supply Dutch patients with pharmaceutically approved cannabis. Canadian patients are also critical of the strength of the cannabis they receive. However, I do not believe that strength is the main issue. Patients who used to buy medicinal cannabis illegally in the Netherlands expressed satisfaction with a content of 10 percent, although stronger varieties were also available. I have no illusions on this score. Dutch patients are also critical, and it will be impossible to satisfy everybody. The point is that we know so little at present and it will take several years to obtain the information we need to produce the best possible treatment for specific conditions. The Canadians are also dissatisfied with the price of cannabis, which I consider quite low. Although we market our products at cost price, they are twice as expensive in the Netherlands. It is expensive to produce cannabis that meets all pharmaceutical requirements. Standardization, laboratory testing, professional packaging, pharmacy services, a 24 hour delivery service countrywide, plus a 6 percent sales tax make prescription cannabis far more expensive than the illegal product. On the other hand, our product is constant in strength and available at all Dutch pharmacies. But the two products cannot be compared. And if we regard it as a medicine, cannabis is not expensive. To its credit, Canada is one of very few countries to fund clinical trials. The results of their research will be invaluable, and I wish we could afford to do the same in the Netherlands. However, we are in the throes of an economic recession and the government is not funding cannabis research. As a result, almost no research is being done. More information will be available shortly on www.cannabisoffice.nl. The Dutch site, www.cannabisbureau.nl is now open. Do you feel competition from the coffee shops or other illicit distributors? James Burton: Not at all. We produce a medicine. As medicines go, this is a very affordable choice. The dangers of the illegal product are the same everywhere: no idea of potency, how it was grown and what contaminates it might contain. We deliver a safe medicine to people who would never buy from a coffee shop Would you comment on the reported criticism of the newly released Canadian cannabis. James: There is no reliable THC testing. Regardless of your methods, testing can be manipulated. Given a certain target and access to a lab, it is conceivable that one could pick the % you wanted to test out at. Using HPLC for instance will always show THC levels 3 to 5% higher. HPLC 高速液体クロマトグラフィー(High performance liquid chromatography) will give you a different reading than testing by 液体クロマトグラフ質量分析計(LC-MS)MSGS http://www.an.shimadzu.co.jp/products/lcms/lcms.htm Each method will give you a different reading on the same sample. Even though this is one of the most studied plants on the earth we know so little about some things. We are still learning about pre-heat temperatures and cannabinoid vaporization levels. The most insidious mistake that Canada has made, and likely contributing factor to this situation is the further stigmatization of an already highly stigmatized issue. Becoming the direct distributor of cannabis is without precedent and sends the message to patients that this plant is even more dangerous than any other chemical drug, and so dangerous that it can only be managed by the government. To receive a normal medicine, you do not have to fill out special government forms. I am aware that Canada was forced to act by the courts, but they did have some choices. Now they have created a situation where the patients have to choose who they trust more, their government or their dealers. So tell me more about the issue of quality James: Quality is in the whole process, the growing, trimming, curing handling and storage. Getting rid of the chlorophyll is just the start, we use dark and temperature and time not unlike a wine maker to bring out the best of the strain. I refer to what I call my cookbook which contains formulas for each strain or cultivar. In it I have the plant and strain specific organic nutrient and other environmental variables required to produce a perfect healthy plant in dirt. Regardless of the lighting companies claims of wide spectrum coverage, real sunshine is still the healthiest and the best for both the plant and the people who use it. I have heard some conflicting reports on the acceptance of cannabis as a medicine by the insurance companies? James: In Holland, the more affluent who have private insurance will have the cost of their cannabis covered under their insurance, but those on the public plan are not at this time covered. I would predict that they will be include in the next few years. Looking forward a few years, where are you going? James: I have a few old cannabis medicine bottles from the early 1900s and I remind my friends that this is not new, this is the reintroduction of an old medicine. I see our cannabis industry creating a vigorous and healthy debate and I predict over the next 2 or 3 years, you will see increasing levels of acceptance of medical cannabis in the European community and new opportunities for our company and others. Can you comment further on your relationship to the Canadians? James: We have had a number of visits and an ongoing relationship with our Canadian officials We were disappointed that Canada did not take us up on the offer we made to assist them with their start up. We offered some genetically stable seed strains and if they wished for even more control, we offered to share cloned stock. The option to acquire Dutch cannabis was also available. I am not aware of what seeds were finally chosen. Patients assisted in the selection of cultivars that were chosen for distribution here, and we even offered to supply Canada with cannabis grown in Holland to make it possible for them to begin research. SIMM Frequently Asked Questions Where is SIMM located? The exact location of the SIMM growing facility is kept private, for obvious security reasons. Is it possible to make a personal visit to SIMM for information gathering purposes? It is not possible for individual patients to visit the facility. Nor are we open for visits from the general public. Press visits and interviews can be arranged in advance. Please see the contact information page. Is it possible to order medical cannabis through the Internet? No, that is not possible. Is it possible to order the SIMM 18 directly from us? Not at this time. How many varieties of cannabis are produced? We have produced as many as 134 different types of cannabis at our facility. Why so many varieties? SIMM believes that patients may find one particular variety more beneficial than another variety. For this reason, patients are able to choose among many types to select the one that is most effective. What price did you charge patients for the medical cannabis which you distributed directly to them? Most of the varieties were priced at EURO 3,00 per gram. For a few of the varieties which required a longer flowering time, the price was higher, at EURO 4,00 per gram. Was it necessary for patients to have a doctor’s prescription before you provided them with cannabis? Yes, a prescription was always required. Were you “legal” when you were providing to patients from 1993 through September of 2003? No, we were not legal, but we were tolerated. Law enforcement officials were aware of our activities and our growing location. What growing method (biological or hydroponic) do you use for producing medical cannabis? SIMM has always grown organically, in soil. Use of fertilizers is kept to a minimum, using only what the plants require. Use of pesticides is very limited. SIMM believes in growing under natural sunlight, supplemented by artificial lighting when required. How can the cannabis prescribed by the doctor be used by the patient? Although smoking of cannabis is the most widely used method, vaporization is strongly recommended. It is possible to make tea, or to add cannabis to other milk (chocolate) products for example. Why is the price of the SIMM 18 in the pharmacies so high? SIMM has no control over the price which is placed on the pharmacy cannabis. This is set by the Bureau voor Medicinale Cannabis of the Ministry of Health in The Netherlands. |



De Cannabis Apotheekハンツェプレイン薬局
オランダ厚生省医療カナビス局
メディカル・マリファナ・スティヒチング研究所(SIMM)
ベドローカン

医療カナビスの知識の普及を目指すオランダ医療カナビス協会が発足 (2008.12.28)オランダの製薬会社、5年以内のカナビス・ピル販売に照準 (2008.1.23)
オランダ、カナビス・ベース医薬品の開発を推進 (2007.11.7)
オランダで初の医療カナビス専門薬局 (2006.12.10)
オランダ政府の医療カナビス、カナダ・ドイツ・イタリアが購入打診 (2006.11.26)
オランダ控訴審、医療カナビスの個人栽培を認める (2006.10.21)
オランダ政府、安価な医療カナビス提供に再挑戦 (060202)
オランダ政府、医療カナビスの販売中止へ、売上げ不振で思惑外れる (2005.6.7)
医療マリファナ配布事業中止へ、オランダ政府 (2005.3.18)
オランダ患者、薬局よりコーヒーショップ (2005.2.7)
オランダ政府のポット売れず (2004.10.13)
薬局ウイードは高くて効かず (2004.2.21)
医療マニュアルはどこに? 医療ユーザーのウイード・テスト (2003.9.9)
オランダ政府、医療カナビス販売開始 (2003.9.1)
オランダ、医療カナビス処方開始、コーヒーショップのメディウイードは不要に (2003.8.30)